Meaningful Use Stage 2 Requirements
Update: The Meaningful Use program was renamed in 2018 to the Promoting Interoperability program to highlight CMS´ focus on interoperability between health IT systems and improving patient access to health information. The new program was effectively Meaningful Use Stage 3.
In 2022, CMS discontinued the Medicaid Promoting Interoperability Program. Eligible clinicians that previously participated in the Meaningful Use and Promoting Interoperability incentive programs are now required to participate in the Merit-based Incentive Payment System (MIPS).
XXXXXXXXXXXXXXXXXXXXXXXXXXXX
Progression from Meaningful Use Stage 1 to Stage 2 requires eligible professionals (EPs), Eligible Hospitals (EHs), and Critical Access Hospitals (CAHs) to have satisfied the core objectives and other Meaningful Use Stage 1 requirements for two years, with progression to Stage 3 requiring 2 years of meeting Meaningful Use Stage 2 requirements.
Get The FREE
HIPAA Compliance Checklist
Immediate Delivery of Checklist Link To Your Email Address
Please Enter Correct Email Address
Your Privacy Respected
HIPAA Journal Privacy Policy

Meaningful use requirements are cumulative, so as EPs, CHs, and CAHs progress through the stages, they are required to continue to demonstrate meaningful use of the objectives of the previous stages, on top of meeting the additional objectives of the new stage.
The aim of Stage 1 was to implement EHRs and their associated technology, to meet 15 core objectives – 14 for EHs and CAHs – and achieve a minimum threshold in those objectives, satisfy five menu objectives and six clinical quality measures.
Meaningful Use Stage 2 Requirements
The Meaningful Use Stage 2 requirements differ slightly from those in Stage 1. Some core objectives have been combined and others eliminated, although most continue in Stage 2. The difference for Stage 2 being an increase in the minimum thresholds that must be achieved.
While Stage 1 involved the basic use of EHRs, Meaningful Use Stage 2 requirements are more focused on using EHRs to improve quality of care, with the three main priorities being clinical decision support, patient and family engagement, and documenting continuity of care decisions.
Meaningful Use Stage 2 requirements for EPs involve meeting 17 core objectives, three menu objectives from a list of six, or 20 core objectives. CAHs and EHs are required to meet 16 core objectives and 3 menu objectives, or a total of 19 core objectives in order to receive Stage 2 incentive payments.
Meaningful Use Stage 2 Core Objectives
The additional core objectives for Stage 2 relate to electronic messaging. EPs must use secure electronic messaging to communicate relevant health information with patients, while EHs and CAHs must track medications automatically from order to administration using assistive technologies, in combination with electronic medication administration records. These new core objectives are intended to benefit patients by improving safety and care.
Some of the core objectives required in Stage 1 have been altered for Stage 2. One of the core objectives in Stage 1 was to provide patients with electronic copies of health information on request. In Stage 2, this changes to providing patients with electronic copies of health information online. The timescale for providing access to online health information differs for EPs and EHs/CAHs. EPs have to provide access within 4 days of the request being received, while EHs/CAHs have to provide access to online health information within 36 hours of discharge from the hospital. In both cases, patients must have the ability to view, download, and share their health information. More than 5% of patients seen by the EP – or admitted as an inpatient/seen by the emergency department – must view, download, or share their health information.
In Stage 1, EPs, EHs and CAHs were required to exchange key clinical information with providers of care when patients transitioned or were transferred to other providers in at least 50% of cases. Stage 2 also requires summaries of care provided to be issued electronically for more than 10% of transitions/referrals.
Further, when a patient is referred or transitioned to another care provider, it is necessary to conduct at least one successful electronic exchange of a healthcare summary with a recipient using technology designed by a different EHR developer than that of the sender of the information. Alternatively, it is necessary to run at least successful one test with the CMS designated test EHR during the reporting period.
While Stage 1 required reporting on clinical quality measures, this requirement is removed from the core objectives in Stage 2 although to demonstrate continued meaningful use, all providers must report on CMQs from 2014. EPs are required to report on 9/64 CQMs and EHs and CAHs are required to report on 16/29 CQMs.
Those CQMs must be selected from at least three of the six healthcare policy domains listed below:
- Clinical Processes/Effectiveness
- Efficient Use of Healthcare Resources
- Population and Public Health
- Care Coordination
- Patient Safety
- Patient and Family Engagement
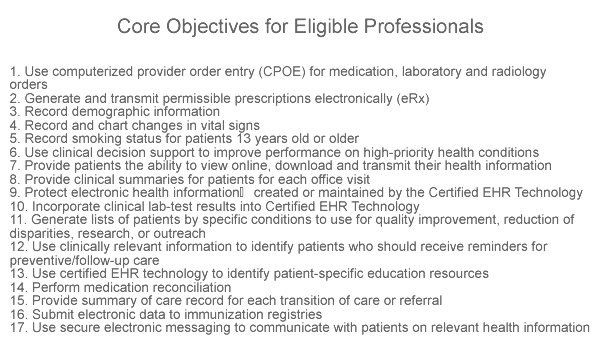
Meaningful Use Stage 2 Requirements – Core Objectives for Eligible Professionals (17/17)
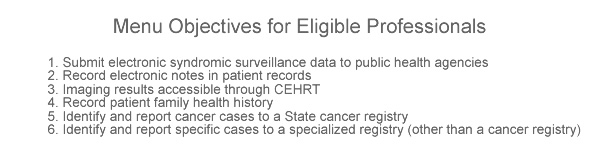
Meaningful Use Stage 2 Requirements – Menu Objectives for Eligible Professionals (3/6)
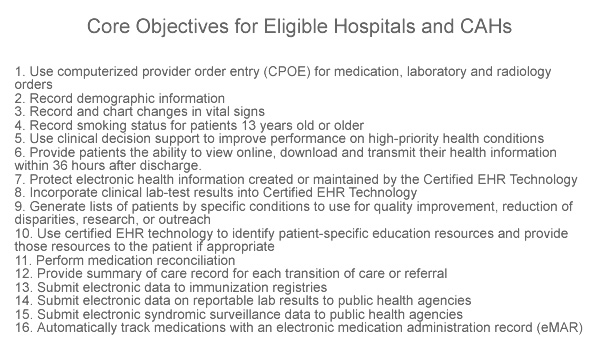
Meaningful Use Stage 2 Requirements – Core Objectives for Eligible Hospitals & CAHs (16/16)
Meaningful Use Stage 2 Requirements – Menu Objectives for Eligible Hospitals & CAHs (3/6)
Timeline for Meeting Meaningful Use Stage 2 Requirements
The Meaningful Use program commenced in 2011, so the earliest that an eligible professional / eligible hospital could progress to Stage 2 was in 2013. However, the CMS delayed the start of stage 2 until 2014, so any provider that started in 2011 is required to continue to meet Stage 1 objectives for a further year.
The timeline for meeting the requirements of Stage 2 depend on the first payment year, as detailed in the table below:
|
Stage of Meaningful Use by First Payment Year |
|||||||||||
| First Payment Year |
Meaningful Use Stage |
||||||||||
| 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | |
| 2011 | 1 | 1 | 1 | 1 or 2 | 2 | 2 | 3 | 3 | TBD | TBD | TBD |
| 2012 | 1 | 1 | 1 or 2 | 2 | 2 | 3 | 3 | TBD | TBD | TBD | |
| 2013 | 1 | 1 | 2 | 2 | 3 | 3 | TBD | TBD | TBD | ||
| 2014 | 1 | 1 | 2 | 2 | 3 | 3 | TBD | TBD | |||
| 2015 | 1 | 1 | 2 | 2 | 3 | 3 | TBD | ||||
| 2016 | 1 | 1 | 2 | 2 | 3 | 3 | |||||
| 2017 | 1 | 1 | 2 | 2 | 3 | ||||||
Meaningful Use to MIPS: FAQs
What is MIPS
MIPS stands for the Merit-based Incentive Payment System – a healthcare quality payment program that was introduced in the Medicare Access and CHIP Reauthorization Act of 2015. MIPS consolidates three incentive programs into one – the Meaningful Use/Promoting Interoperability program, the Value Based Payment Modifier, and the Physician Quality Reporting Program.
Who is eligible for MIPS?
MIPS eligibility is dependent on clinician type, the date enrolled in Medicare, and the volume of care provided to Medicare patients. The volume thresholds for 2022 are
- Bill more than $90,000 for Part B covered professional services under the Physician Fee Schedule (PFS), and
- Provide services to more than 200 Medicare Part B patients, and
- Furnish more than 200 covered professional services to Part B Medicare Patients.
If a physician fails to meet the thresholds, can they still participate in MIPS?
Individual physicians can still participate if the practice at which they work exceeds the threshold. Alternatively, they can elect to join a “virtual group” subject to certain conditions. For example, physicians can join a virtual group of up to nine further clinicians, provided one of the clinicians is MIPS-eligible.
What is the Advancing Care Information program?
The Advancing Care Information program was one of the names suggested for the Promoting Interoperability program. Because it appeared in a number of CMS publications at the time, the name is still used in some sources to explain the EHR incentive portion of the Merit-based Incentive Payment System.
How does MIPS incentivize participants?
MIPS incentivizes participants by offering a bonus to Medicare Part B payments based on the quality of care, improvement activities, promoting interoperability, and cost of service. CMS frequently runs campaigns that can increase or reduce scores in certain categories – for example, the Hospital Readmission Reduction Program.